
Assessment of Acute Knee Injuries
History: Determine the exact mechanism of injury to help predict the possible extent of damage to the knee. It is important to know the position of the knee at the time of injury, the magnitude of the forces and direction applied to the knee.
An RTA or fall from a height is likely to generate massive forces capable of rupturing ligaments and fracturing bone. Football is a knee disease with a high frequency of ligamentous injury. Skiing can apply great force to the knees if the skis get crossed or stuck and the body continues with considerable stored momentum! Patients and bystanders often report an audible crack/pop/snap indicating a sudden release of energy as something fails under load.
A history of prodromal symptoms in the knee suggests wear which may have been exacerbated by the current injury. Progressive aching and joint-line tenderness before developing a locked knee is usually due to a degenerative meniscal tear. Repeated episodes true-locking suggests a large meniscal fragment or a loose body in the knee.
Disability: Inability to bear any weight on the leg immediately after an injury suggests some serious pathology. A gradual onset of swelling and discomfort leading to limping and reduced weight bearing suggests swelling is limiting activity, rather than a mechanical failure in the knee.
Patients unable to walk/drive/work benefit from early treatment either by referral to physiotherapy or to the knee clinic.
Examination:
LOOK - Compare the two sides and note malalignment, swelling, bruising and any wounds. Intra-articular swelling will be limited by the capsule of the knee (unless the capsule has been ruptured, for example in a knee dislocation). A haemarthrosis may be very tense and limit any movement. Only structures with a good blood supply can cause an acute haemarthrosis (e.g. ACL Rupture, PCL Rupture, Peripheral Meniscal Detachment and Intra-articular fractures such as Tibial Plateau Fractures )
Do not confuse intra-articular swelling due to injury, with pre-patella bursitis which is usually inflammatory and occasionally infective: -

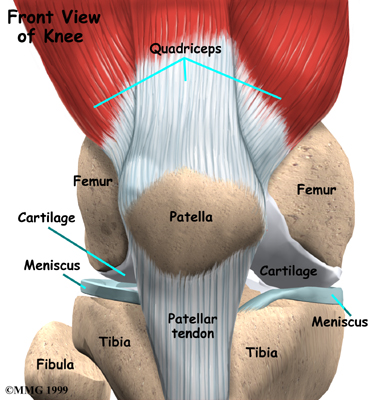
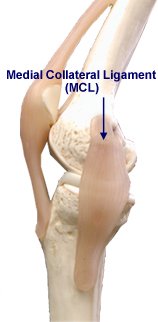
FEEL - Look through the skin to understand what you are palpating. Note tenderness of the bones, ligaments and meniscii.

MOVE - Compare the two sides for passive range, active movement and ligamentous stability.
Imaging:
As with all investigations imaging should only be used to aid decision making:-
For high energy knee joint injuries plain x-rays must be undertaken before referral to the knee clinic. MRI scanning is not always necessary and patients should not be told this "will be required".
© Mr Gavin Holt :: CotswoldClinics.com :: Print this frame