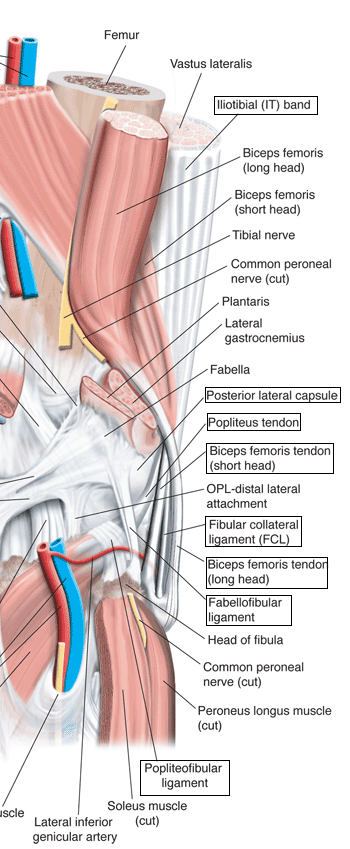
Structures of posterolateral corner (PLC) The lateral side of the knee is best considered in three layers:- Superficial
Middle
Deep (two portions): Fibular Collateral Ligament
Arcuate Complex
|
(Posterior aspect right knee)
|
Posterolateral Corner Injuries
The posterolateral corner encompasses all the structures on the lateral side of the knee. There are many different ligaments and therefore a number of different injury patterns. Isolated PLC injuries are rare and combined injury of the PLC with the ACL and particularly PCL are common. In cases of combined injury, a knee dislocation which has spontaneously reduced should be considered.
As the forces required to damage the PLC are of a similar magnitude to those causing knee joint dislocation it is not surprising that neurovascular injury can occur:-
The posterolateral corner structures act with the ACL to stabilize the lateral compartment of the knee. The "medial pivot" model for knee joint kinematics implies that the lateral compartment has much more laxity than the medial compartment, both in translation and rotation. As such this compartment cannot have isometric ligaments and instead has "check reins" creating an envelope of permissible movements.
For the knee as a whole the PLC controls: -
The LCL has been reported to be injured in only 23% of PLC injuries1, therefore the absence of varus laxity should not be used to exclude damage in this area.
The lateral side of the knee, including the posterolateral corner, is stabilized by a number of static and dynamic structures that prevent pathological translation, rotation, and angular motion. Seebacher et al2 used the layer concept to divide the lateral structures into three distinct layers from superficial to deep.
Structures of posterolateral corner (PLC) The lateral side of the knee is best considered in three layers:- Superficial
Middle
Deep (two portions): Fibular Collateral Ligament
Arcuate Complex
|
(Posterior aspect right knee)
|
Diagnosis
Hx |
|
LOOK |
|
FEEL |
|
MOVE |
Exclude combined PCL + PLC
Exclude combined ACL + PLC
|
XRAYS |
AP and Lateral views
|
MRI |
For all potentially multiple ligament injuries
|
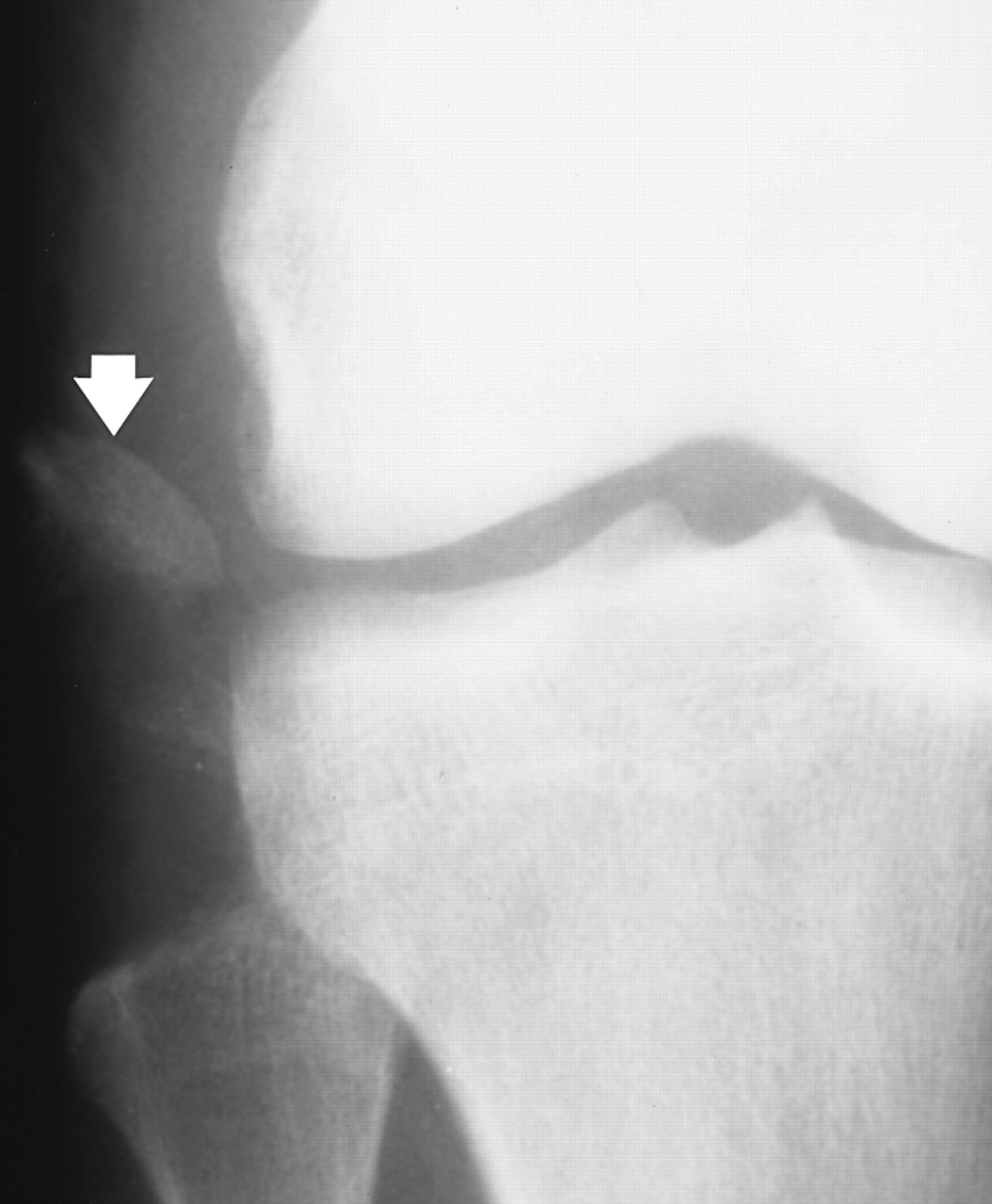
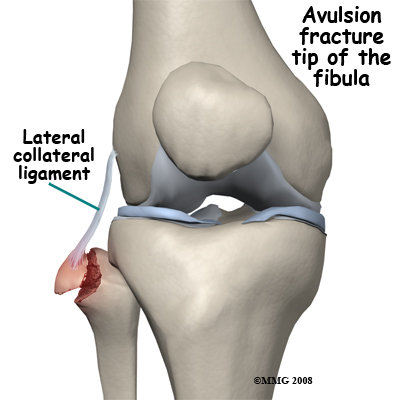
This injury must be suspected in all high grade ACL or PCL injuries: -
Avulsion fractures are common and easily missed. This may involve the lateral epicondyle, a Segond capsular avulsion or occasionally there is a tell tale avulsion of the tip of the fibular head indicating distraction of the lateral ligaments, this is termed the "Arcuate sign".
Emergency Room Treatment
Many of these patients will have multiligament injuries and will need an emergency orthopaedic referral.
© Mr Gavin Holt :: CotswoldClinics.com :: Print this frame