Introduction
Sacroiliitis is an inflammation of one or both of the sacroiliac joints. This may be mechanical wear and tear, however sacroiliitis is strongly linked to spondyloarthropathies (inflammatory arthritis of the spine). This condition may be the presenting complaint and therefore an accurate diagnosis is required.
Anatomy
The upper posterior ligamentous portion is a space in which the sacrum and ilium are not in contact, while the anterior and lower half is a typical synovial joint lined with hyaline cartilage. This is a sliding joint with motion too small to measure although. The sacroiliac joint has an extensive nerve supply is from L2 to S3 (Hilton's Law) and pain may be referred to the groin, or distally into the leg as an ill-defined sensation radiating to the toes.
Clinical Features
Sacroiliitis can be difficult to diagnose because it may be mistaken for other causes of low back pain. Sacroiliitis can cause pain in the buttocks or lower back, and may even extend down one or both legs. The pain associated with sacroiliitis is often aggravated by prolonged standing, by stair climbing and pain on turning over in bed is common.
Patients may well point to the affected area; below the iliac crest in the sacroiliac sulcus. This area may be locally tender. Contrast this with facet pain where the finger usually points above the crest and sciatica where a full radicular pattern will be demonstrated.
The FABER test (Flexion Abduction External Rotation; aka Patrick's Test) will precipitate pain. Similarly the sacroiliac joint can be stressed with a "Posterior pelvic thrust Test" pushing the flexed knee into the hip in the 90/90 position. There should be no radicular signs indicating nerve compression (i.e. -ve Sciatic Stretch Test/Femoral Stretch Test, Normal Passive Straight Leg Raising, Normal Tone/Power/Sensation/Coordination). Hip examination is undertaken to exclude other sources of pain.
Other diagnoses must be excluded before any direct treatment is indicated:-
Investigations
Inflammatory markers are measured to identify spondyloarthropathies with full blood count and differential white count to exclude infection. Simple radiographs are made to check for lumbar degeneration or hip pathology. MRI of spine will exclude spinal nerve compression and other spinal pathology. MRI of hips may be necessary to check for occult pathology (Labral tears, AVN, early OA).
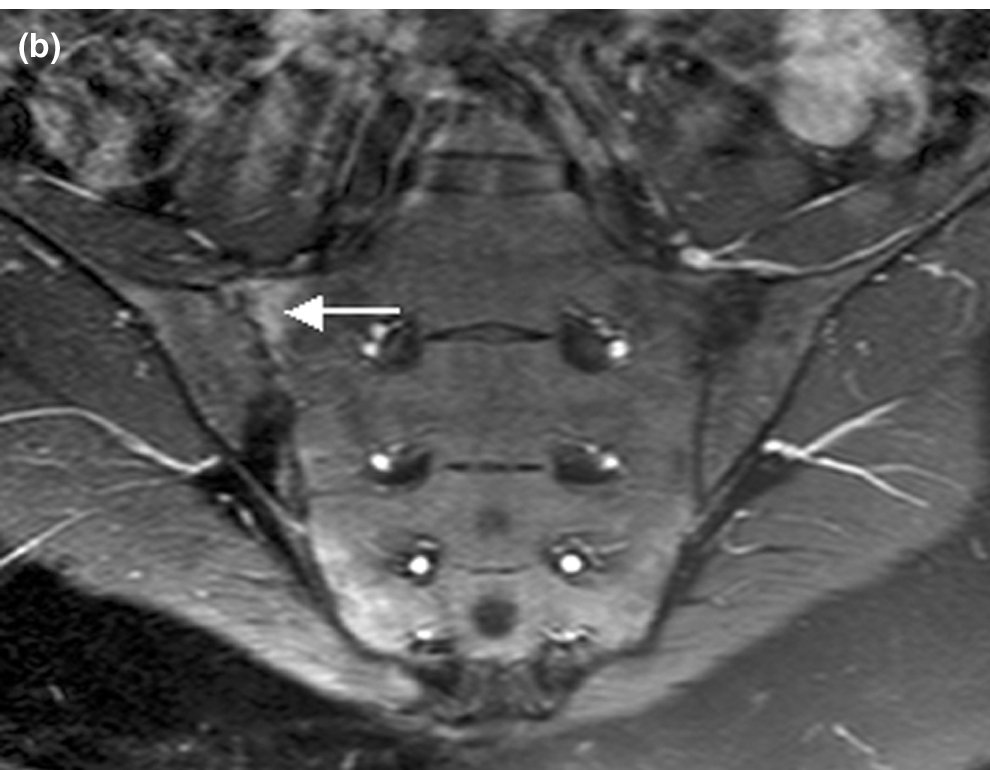
The sacroiliac joints can be imaged using MRI, mainly to exclude unusual pathologies (Infection, Stress Fracture).
Treatment
Mechanical sacroiliitis should respond to simple analgesia, weight loss and physiotherapy. Occasionally help is required from the Chronic Pain Team.
© Mr Gavin Holt :: CotswoldClinics.com :: Print this frame