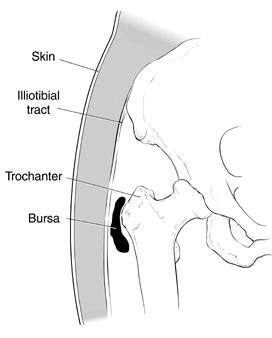
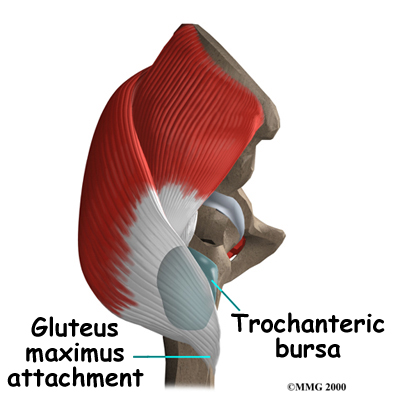
The greater trochanter is the prominent piece of bone situated at the upper outer aspect of the femur, as is palpable in most people just to the outer side of where a trouser pocket starts. The bone is enlarged where a large mass of muscles (the hip abductors) attach to the femur. One strong muscle (Tensor Fascia Lata) by-passes the hip to attach below the knee.
The bursa is a sack of fluid, which acts a lubricator between the muscle and the underlying trochanter. Bursae are found in many sites around the body; typically between areas of bone or tendon and the skin. The function of a bursa is to minimise potential rubbing and friction between two tissues.
The trochanteric bursa is found just lateral (to the outside) of the hip joint, beneath the skin, the fat and the facia lata, just superficial to the muscle layers of the gluteus medius and the vastus lateralis, where they attach to the bone.
Clinical features
Trochanteric bursitis may come on after trauma, repetitive micro-trauma (overuse), in the presence of osteoarthritis, or even after a hip replacement. Many times, no specific cause can ever be clearly identified.
When a bursa becomes inflamed, the condition is referred to as 'bursitis', the area becomes tender and painful. The region may become hot, red and swollen. However, with certain deep bursae (such as the trochanteric bursa), these superficial signs may not be apparent.
Trochanteric bursitis normally causes a sharp or burning pain over the lateral (outside) side of the hip. The pain may radiate down the lateral side of the thigh towards the knee. The pain is usually made worse by walking or trying to run. The most pathognomonic symptoms and signs are tenderness over the lateral side of the hip, plus pain when trying to lie on that side in bed. This pain often interferes with patients' sleep.
Investigations
Diagnosis is often clear from simple history taking plus clinical examination. However, in cases where the diagnosis may not be entirely clear or where more definite confirmation is desired, then the investigation of choice is an ultrasound or MRI scan of the hip.
In addition, it is sometime appropriate to perform further investigations such as X-rays, to exclude the potential presence of osteoarthritis of the hip, or MRI scans, if other hip pathology such as a labral tear is suspected.
Management
The first step in the treatment of trochanteric bursitis is to try rest plus anti-inflammatories. Some patients' symptoms may be helped by physiotherapy treatment to stretch out the "pelvic deltoid".
For persistent cases a local anaesthetic plus cortisone injection into the bursa usually helps. The cortisone is a very powerful anti-inflammatory and normally works very well, although it may sometimes be necessary to repeat the injection more than once. The injection can either be given directly in the outpatient clinic, or, in those patients where the bursa is felt to be too deep within the tissues, ultrasound-guided injection in the X-ray department may be appropriate.
Surgery
In that very small proportion of patients where all other treatment options fail and where the symptoms remain severe, surgical excision of the bursa is very occasionally necessary. This is an open operation, performed normally under a general anaesthetic. The operation lasts only 20 or 30 minutes, but the dissection does go quite deep. Therefore, there can be significant post-operative discomfort, and patients normally need to stay in hospital post-operatively for a day or two. The wound normally takes only a week or so to heal, but the deeper tissues may take up to 6 weeks to settle, during which time some patients may require a walking stick initially, to help them walk, followed by a course of physiotherapy to help them regain their strength and motion.
© Mr Gavin Holt :: CotswoldClinics.com :: Print this frame