This refers to inflammation, partial tear or complete rupture of the iliopsoas muscle and tendon along with iliopsoas bursitis. It is rare for the iliopsoas muscle-tendon to rupture completely. Iliopsoas tendinitis and iliopsoas bursitis are closely interrelated because of their close proximity inflammation of either inevitably causes inflammation of the other. Iliopsoas tendinitis and iliopsoas bursitis are essentially identical in terms of presentation and management.
Clinical features
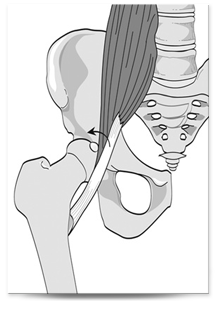
Presentation may include groin pain with an associated snapping sensation. Very occasionally there is a palpable mass, or a compression syndrome of the inguinal compartment secondary to enlargement of iliopsoas tendon and associated bursae.
Symptoms include pain after onset of aggravating activity with resolution soon after ending the activity, the condition may progress to pain that persists during activity but subsides some time after with rest. Eventually it progresses to pain during activity and at rest.
This condition may occur if there is an overuse phenomenon associated with repeated hip flexion or external rotation of the femur e.g. in professional dancing, pain may occur with specific sports-related activities, such as running or kicking as in football. There may be pain with other simple activities such as putting on socks and shoes in the severe cases.
Physical examination
Often reveals localized tenderness in the area of the inguinal ligament and pain with resisted hip flexion or passive hyperextension.
Ludloff sign: The patient asked to sit with knees extended and subsequent elevation of the heel on the affected side pain caused by this manoeuvre (a positive Ludloff sign) is consistent with an iliopsoas tendinitis - this is because iliopsoas is the sole hip flexor activated in this position.
The affected hip in a flexed, abducted, and externally rotated position (with the knee flexed) - the hip is then moved passively into extension this test may cause an audible snap or palpable impulse over the inguinal region.
Investigations
MRI scan is the imaging modality of choice for diagnosing this problem, although ultra sonography can be useful if an enlarged bursa is present.
Management
Non operative treatment, including rest, non steroidal anti-inflammatory medications, and a stretching exercise program, has been recommended for the treatment of this condition. Corticosteroid/local anaesthetic injection is a non operative management option that may be required if the exercises have no effect.
Iliopsoas muscle injury can cause lumbar lordosis and anterior pelvic tilt, these can be corrected by strengthening by strengthening the abdominal musculature, sit-ups or crunches executed with knees and hips flexed at 90° allows the iliopsoas to relax, with the effort concentrated on the rectus abdominus muscle.
Surgery
Surgical release of the iliopsoas tendon, procedure may be undertaken if non operative treatment has failed. This can be performed as an open procedure or arthroscopically allowing examination of the peripheral compartment of the hip joint. Once the iliopsoas tendon is located it can be partially released to take off the tension and stop the catching and reduce the symptoms. The release is done at the level of the head neck junction or at its insertion into the lesser trochanter.
© Mr Gavin Holt :: CotswoldClinics.com :: Print this frame