Branches of the obturator nerve:- Anterior division
Posterior division
|
Branches of the obturator nerve:- Anterior division
Posterior division
|
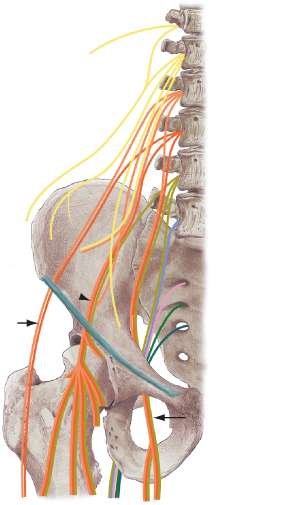
Anterior branches of the anterior primary rami of L2, L3, and L4 fuse to form this nerve. The major contribution is from L3, and the least amount of contribution typically is from L2. The rami fuse in the substance of the psoas muscle and emerge from the medial border of the psoas beneath the common iliac vessels just lateral to the sacrum. The obturator nerve then travels along the lateral wall of the true pelvis to enter the obturator foramen. Just anterior to the internal obturator muscle and prior to entering the thigh, the nerve divides into an anterior and a posterior branch.
The anterior branch travels superficial to the internal obturator muscle but deep to the pectineus and adductor longus muscles and then travels superficial to the adductor brevis muscle. Motor branches arise just distal to the obturator foramen to supply the adductor brevis, adductor longus, and gracilis muscles. In keeping with Hilton's Law there are articular branches to the hip joint. The nerve terminates at the distal aspect of the adductor longus by forming a subsartorial plexus by communicating with the medial cutaneous branche of the femoral and the saphenous nerve. Rarely, a terminal cutaneous branch may emerge from the inferior aspect of the adductor longus muscle and follow the medial border of the sartorius muscle to the medial knee region, where it supplies the skin of the medial and distal thigh region.
The posterior branch pierces obturator externus and passes down behind the adductor bervis and in front of adductor magnus. It terminates by descending through the adductor hiatus to supply an articular branch to the knee joint.
Entrapment may occur in the obturator canal during surgery or with total hip arthroplasty. Other potential causes include malposition of the lower limb for prolonged periods (lithotomy), entrapment in the adductor magnus in athletes, and abnormal positioning of the lower limb of a newborn during a difficult delivery. Some physicians believe that the anterior branch may be entrapped in the fascia as it passes over the adductor brevis muscle, owing to an inflammatory process.
The obturator nerve is rarely directly injured in isolation. However, injury can occur with pelvic trauma and associated fractures, during delivery as a result of compression of the nerve between the head of the fetus and the bony structures of the pelvis, or as a consequence of compression of the nerve between a tumour and the bony pelvis.
The main complaints in obturator entrapment include difficulty with ambulation and the development of an unstable leg. In an anterior branch entrapment, symptoms can consist of exercise-related pain or groin pain. The patient may describe a deep ache in the region of the adductor origin at the pubic bone that increases with exercise; the pain may radiate down the medial aspect of the thigh toward the knee. An athlete's ability to jump may weaken. The weakness in these patients usually worsens with exercise.
With severe injuries, loss of adduction and internal rotation occur, and the typical gait pattern is that of an externally rotated foot. Examination reveals wasting of the adductor muscles of the thigh and possibly diminished sensation along the medial thigh distally. The differential diagnosis includes adductor muscle strain, osteitis pubis, stress fracture of the pelvis, enthesopathy, entrapment of the lateral cutaneous nerve of the thigh, and inguinal hernia.
No routine conduction studies are available with which to evaluate the integrity of the nerve, and the needle examination is the mainstay of testing with electrodiagnosis. Membrane instability (positive sharp waves and fibrillation potentials) will occur within 3 weeks of the nerve injury, and needle examination should be performed on patients with groin pain of longer than 3 months in whom this neuropathy is suspected. Complete injury results in a lack of active motor unit potentials. Muscles from the quadriceps (femoral nerve), as well as the paraspinal muscles, must be examined and found to be normal before an obturator nerve injury can be diagnosed. In this manner, one must rule out a radiculopathy and a plexus injury as potential causes of the weakness in adduction during the electrodiagnostic examination. A nerve block may be helpful but usually is not necessary for diagnosis.
For anterior nerve entrapment, treatment may consist of electrical stimulation of the adductor and hip flexor muscles, stretching, and massage. These modalities, however, typically have not been successful in resolving this condition if it is not recognized early. For athletes, surgery is the preferred treatment when there is significant disability and electromyography shows denervation. The surgery involves dividing the fascia over the pectineus and the adductor longus muscles and dissecting the space between the two muscles to reveal the anterior branch of the nerve beneath. This fascia is divided along the line of the nerve, and the adductor longus-pectineus junction is closed loosely.
© Mr Gavin Holt :: CotswoldClinics.com :: Print this frame