|
|
Anatomy
|
|
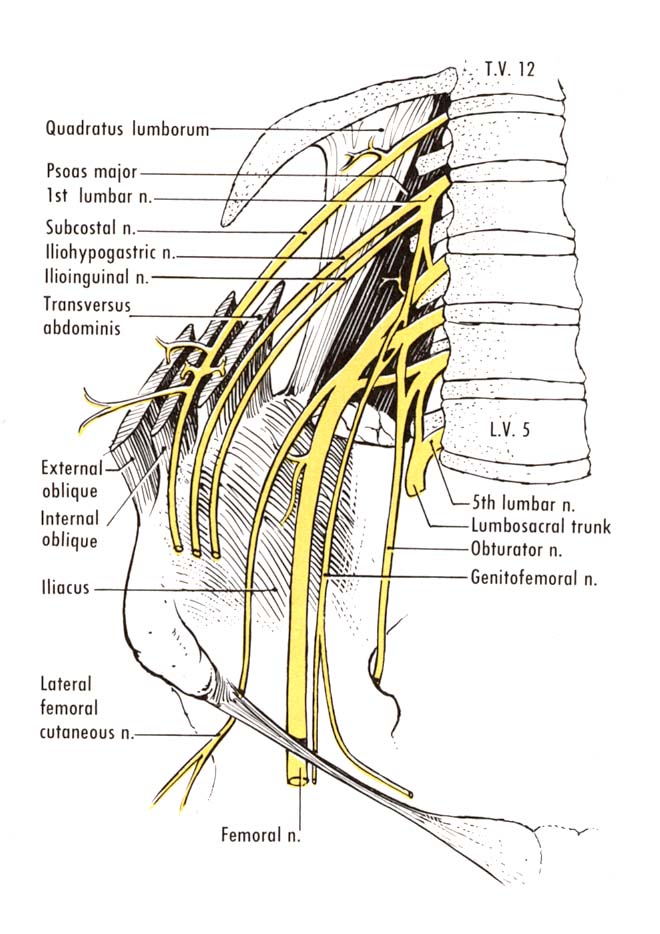
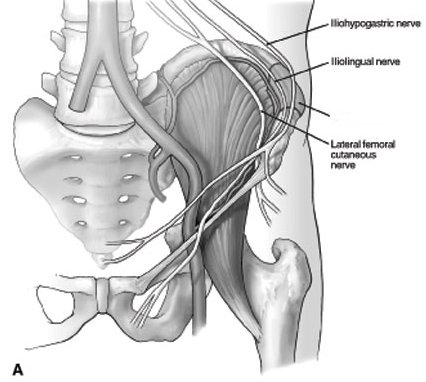
The ilioinguinal nerve arises from the fusion of T12 and L1 nerve roots and emerges from the lateral border of the psoas muscle; it traverses the anterior abdominal wall to the iliac crest just inferior to the hypogastric nerve. Adjacent to the anterior margin of the iliac crest, the nerve pierces the transversus abdominis and internal oblique muscles (providing neural branches to these) and sending neural branches to the iliohypogastric nerve. The nerve then supplies sensory branches to supply the pubic symphysis, the superior and medial aspect of the femoral triangle, and either the root of the penis and anterior scrotum in the male or the mons pubis and labia majora in the female.
Aetiology
Causes of injury include lower abdominal incisions (Pfannenstiel), pregnancy, iliac bone harvesting, appendectomy, inguinal herniorrhaphy, inguinal lymph node dissection, femoral catheter placement, orchiectomy, total abdominal hysterectomy, and abdominoplasty. The prevalence of injury with surgery has declined, owing to the use of laparoscopic procedures.
Tearing of the lower external oblique aponeurosis may also cause injury to this nerve. This injury has been reported in Ice Hockey players.
Symptoms
Symptoms may include hyperesthesia or hypoesthesia of the skin along the inguinal ligament. The sensation may radiate to the lower abdomen. Pain may be localized to the medial groin, the labia majora or scrotum, and the inner thigh. The characteristics of the pain may vary considerably. Patients may be able to associate their pain clearly with a traumatic event or with the surgical procedure.
Pain and tenderness may be present with application of pressure where the nerve exits the inguinal canal medial to the anterosuperior iliac spine (ASIS). Sensory impairment is common in the above-noted distribution of the nerve supply. Symptoms usually increase with hip extension (patients walk with the trunk in a forward-flexed posture).
The diagnosis can be made on the basis of local infiltration of anesthetic with or without steroid, which should result in relief within 10 minutes. Unfortunately, no electrodiagnostic techniques are readily available to test this nerve. Abdominal needle electromyography may be helpful in determining the severity of nerve injury, but electromyography is not sensitive or specific.
Treatment
Treatment includes local injection of an anesthetic, physical therapy, or oral medications. Membrane stabilizing medication may help the neuralgia (gabapentin, amitriptyline). A TENS unit may be used with physical therapy. When conservative measures are not successful, surgical excision may result in relief of pain with few potential complications.
© Mr Gavin Holt :: CotswoldClinics.com :: Print this frame